
.webp) 2 weeks ago
6
2 weeks ago
6
Presentation
A 51-year-old woman presented to her primary care provider with concerns of worsening short-term memory and increased difficulty with organizing and planning tasks at home and at work. Physical examination revealed chorea characterized by writhing and shifting movements in the extremities. Family history revealed dementia and balance problems accompanied by depression and temper outbursts at the patient's mother's end of life (no genetic testing was performed). The patient was referred to a neurologist for a comprehensive workup.
Huntington disease (HD) is an inherited, autosomal dominant, relentlessly progressive, fatal neurodegenerative disease characterized by involuntary movements, behavioral impairment, and cognitive decline. The classic signs and symptoms of HD typically affect patients between the ages of 30 and 50 years. On the basis of this patient's history, physical examination, and neuroimaging, her diagnosis is HD, which must be confirmed by genetic testing.
Differential Diagnosis
Several potential diagnoses should be considered on the basis of this patient's presentation.
- Multiple sclerosis: an immune-mediated inflammatory disease that attacks myelinated axons in the central nervous system, destroying the myelin and the axon in variable degrees and producing significant physical disability within 20-25 years in more than 30% of patients. The hallmark of MS is symptomatic episodes that occur months or years apart and affect different anatomic locations.
- Neuroacanthocytosis: a group of genetically heterogeneous disorders characterized by neurologic signs and symptoms associated with acanthocytosis, an abnormality of red blood cells. Neurologic problems usually consist of either movement disorders or ataxia, personality changes, cognitive deterioration, and seizures.
- Systemic lupus erythematosus: an autoimmune disorder characterized by antibodies to nuclear and cytoplasmic antigens, multisystem inflammation, highly variable clinical manifestations, and a relapsing and remitting course. More than 90% of cases occur in women, frequently starting at childbearing age.
- Alzheimer disease (AD): a neurodegenerative disorder marked by cognitive and behavioral impairment that significantly interferes with social and occupational functioning. It is an incurable disease with a long preclinical period and progressive course. In AD, plaques develop in the hippocampus, a structure deep in the brain that helps to encode memories, and in other areas of the cerebral cortex that are involved in thinking and making decisions. However, the typical age at onset of AD is the mid-60s or later.
- Frontotemporal dementia: The presentation of degenerative disease in focal areas of the cerebral cortex is the hallmark of the family of diseases referred to as frontotemporal dementia (also termed frontotemporal lobar degeneration). In recent years, the term frontotemporal dementia has become an umbrella term referring to clinical syndromes of frontal dementia or progressive aphasia. Patients often present with personality changes and problematic behavior.
- Corticobasal degeneration: a sporadic neurodegenerative 4-repeat tauopathy and a pathologically defined entity associated with several clinical phenotypes. The most common phenotype, corticobasal syndrome, is defined by progressive dementia and typically asymmetric parkinsonism unresponsive to dopaminergic therapy, dystonia, limb apraxia, and myoclonus, but these may result from other pathologic entities.
- Parkinson disease: one of the most common neurologic disorders, affecting approximately 1% of individuals older than 60 years and causing progressive disability that can be slowed, but not halted, by treatment. The major neuropathologic finding in Parkinson disease is loss of pigmented dopaminergic neurons of the substantia nigra pars compacta, characterized by tremor, gait impairment, and executive dysfunction early in the disease.
- Dentatorubral-pallidoluysian atrophy: a progressive, autosomal dominant CAG repeat disorder typically characterized by ataxia, myoclonus, epilepsy, choreoathetosis, dementia, psychiatric disturbance, and progressive intellectual deterioration.
- Spinocerebellar ataxia (SCA) types 17 and 27, and occasionally SCAs 2 and 3: a genetically heterogeneous group of autosomal dominantly inherited progressive disorders, the clinical hallmark of which is loss of balance and coordination, accompanied by slurred speech, memory loss, and sometimes with chorea; onset is most often in adult life.
Other disorders that may be considered in the differential diagnosis include:
- Tardive dyskinesia
- Thyrotoxicosis
- Levodopa-induced dyskinesia
- McLeod syndrome
- Pantothenate kinase–associated neurodegeneration
- Wilson disease (although this patient is relatively old to have survived with this diagnosis, and Huntington disease testing should be performed first)
Diagnosis
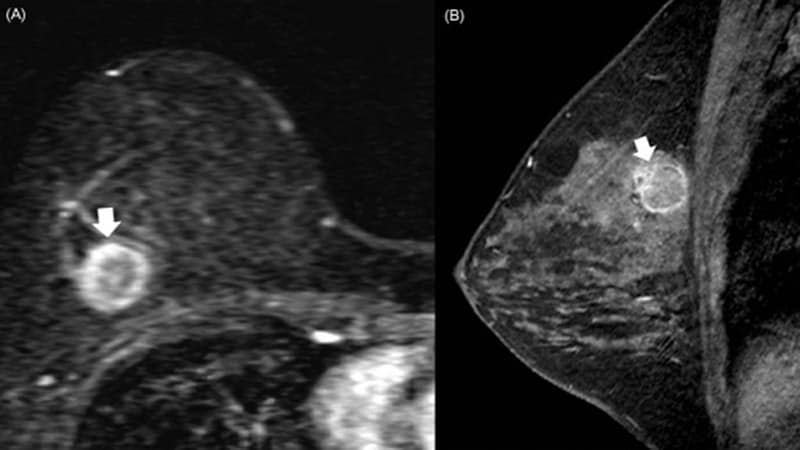
Neuroimaging (brain MRI) showed striatal atrophy in the caudate nucleus.
Genetic testing showed a 43-repeat CAG expansion of the HTT gene.
On the basis of her symptoms, family history, imaging, and genetic testing, the patient was diagnosed with Huntington disease (HD).
Valbenazine was prescribed for management of HD chorea, and the patient was referred to a psychiatrist for medication/therapy to manage the psychological impact of the diagnosis as well as for counseling and educational services. In addition, physical and occupational therapy were recommended for both balance impairment and coordination/dexterity impairment. The patient and her family were also referred to a genetic counselor to discuss the impact of autosomal dominant disease on others who may be at risk for HD.
Physical Examination
Motor signs are characteristic. These include involuntary, typically progressive movements that begin in the distal extremities but can advance to affect the facial muscles and then spread gradually to the more proximal and axial muscles. Initially these are mostly hyperkinetic with involuntary chorea; hypokinesia with bradykinesia and dystonia predominate later. Physical examination of the patient in this case revealed chorea. The balance between chorea and hypokinesia varies from patient to patient and ranges from overwhelming hypokinesis and rigidity in patients with juvenile HD (so-called Westphal variant) to rigidity and contractures of the extremities in older patients. Dysarthria and dysphagia develop during the course of the disease, and dystonia, characterized by increased muscle tone with slower movements, leads to abnormal posturing such as torticollis; it can be the first sign of motor involvement in HD. Other involuntary movements include tics and cerebellar signs such as ataxia. Pyramidal signs such as the Babinski response are characteristically present, together with slowed or interrupted eye movement abnormalities or rapid, jerky conjugate eye movement with shifting gaze across the visual field (saccades) as well as upper limb coordination deficits.
Neuroimaging
No single imaging technique is necessary or sufficient for the diagnosis of HD. However, measurement of the bicaudate diameter (the distance between the heads of the two caudate nuclei) by brain CT or MRI is a reliable marker of HD. Adult-onset HD is typically characterized by early striatal atrophy in the caudate. In the case presented here, brain MRI showed striatal atrophy in the caudate nucleus. Cerebellar and cortical atrophy is seen later in the disease. Atrophy in basal ganglia, particularly in the caudate nucleus, may result in widening of the frontal horns of the lateral ventricle. This appearance on MRI is called the boxcar ventricle sign.
Genetic Testing
HD is caused by expanded CAG (cytosine-adenine-guanine, the trinucleotide coding for glutamine) repeats in exon 1 of the HTT gene, which codes for an abnormal version of the huntingtin protein. Confirmation of more than 40 copies of the CAG repeats in HTT are diagnostic for HD in the setting of HD symptoms, and more than 26 copies is considered abnormal. Genetic testing of the patient in the case presented above identified a 43-repeat CAG expansion of the HTT gene.
The number of CAG repeats present in the HTT gene determines whether an individual will have HD. Those with six to 35 CAG repeats will be unaffected (although, as noted above, more than 26 copies is considered abnormal; such individuals may pass on a longer expansion to any offspring). There are case reports of people with fewer than 36 expansions who develop HD symptoms. Individuals with 36-39 repeats may not develop HD until much later in life, and persons with 40 or more CAG repeats will manifest the disease. In addition, the larger the number of CAG repeats, the greater the rate of deterioration of motor, cognitive, and functional measures on average, although repeat numbers are not useful for making individual prognostic predictions. In one study, individuals with CAG 36-38 repeats had a similar cognitive profile to those with the more common CAG 40-42 expansions. These individuals may evade molecular diagnosis because of the absence of chorea rather than because of a low penetrance of symptoms.
The mutant protein appears to play a role in the progressive neurodegeneration characterizing HD. Persons carrying the mutated allele have a 50% chance of passing this allele to each of their children. Although HD phenotypes usually appear in adulthood, the dominant mutation in the HTT gene is present from birth. Therefore, the genetic test for HD allows the identification of a fully penetrant mutation carrier during the preclinical stage. However, genetic testing is not always necessary when a patient presents with clinical features characteristic of HD in the setting of a known family history. Testing is not recommended for anyone under age 18 unless symptoms suggestive of HD are present. This is to allow individuals to reach a level of maturity and participate in the testing decision themselves.
Staging
HD can be classified by stage of clinical progression from illness onset. Stages of HD can also be categorized on the basis of the extent of striatal pathology, neuronal loss, and gliosis (grades 0-4), based on the original Vonsattel grading system:
- Grade 0: No gross abnormalities or neuropathologic histology despite clinical evidence of HD. There may be up to 30%-40% reduction in neuronal number in the head of the caudate.
- Grade 1: Mild atrophy of the caudate tail and body. The head of the caudate and the putamen may still appear normal. Microscopically, neuronal loss and astrocytosis are predominantly in the tail of the caudate nucleus.
- Grade 2: Some atrophy of the caudate with enlargement of the lateral ventricles, although the ventricular surface maintains its convex shape. The globus pallidus begins to show degeneration.
- Grade 3: Significant atrophy of the caudate, causing the ventricular surface to appear straight as it now parallels the internal capsule boundary. Microscopically, neuronal loss and reactive astrocytosis are visible throughout the caudate and putamen and have become severe.
- Grade 4: Severe atrophy of the striatum causes the ventricular surface to become concave. Microscopically, severe striatal neuronal loss reaches approximately 95% and there is marked astrocytosis. The globus pallidus volume is reduced by half.
Management
Despite the discovery of a genetic mutation as the cause of HD, treatment remains mostly aimed at the relief of symptoms. To date, no effective treatment for preventing the onset or progression of HD is available, and investigational therapies that might slow or reverse disease progression have not been incorporated into routine clinical care. Most symptomatic therapies are vesicular monoamine transporter 2 (VMAT2) inhibitors directed against chorea associated with HD by either depleting dopamine reserves from nerve terminals or blocking dopaminergic receptors in the brain, thereby providing temporary relief to the patient.
Behavioral and psychiatric symptoms have been managed with antidepressants, mood stabilizers, antipsychotics, and psychotherapy, in conjunction with physical, speech and occupational therapy together with supportive care and patient/caregiver education. Cognitive symptoms may be managed with a reduction of medications that impair cognition together with a structured environment. Social work expertise is crucial to providing support for patients and their families, and assisting with disability applications, long-term placement, and provision of other resources.
Seizures may occur in juvenile cases of HD, which are rare, and anticonvulsants (including valproic acid and clonazepam) may reduce seizure frequency.
Various molecular and genetic approaches are being studied in preclinical and clinical trials to reduce levels of mutant versions of HTT or modify clinical features of the disease. For example, antisense oligonucleotides (ASOs) and RNA interference compounds targeting mRNA are huntingtin-lowering strategies currently being studied. In addition, the NMDA receptor modulator SAGE-718 is being studied to assess its safety and effect on cognitive symptoms in patients with HD.
Prognosis
HD is a relentlessly progressive disorder leading to disability and death. The mean age at death in all major series ranged from 51 to 57 years, but the real-world range is broader. Duration of illness varies considerably, with a mean of approximately 19 years. Most patients survive for 10-25 years after the onset of illness.
Clinical Takeaway
HD is a rare, autosomal dominant, monogenic neurodegenerative disorder that presents with progressive symptoms leading to functional decline and motor, psychiatric, and cognitive symptoms, which typically manifest between 30 and 45 years of age. Persons carrying the mutated allele have a 50% chance of passing HD to each of their children. HD risk is associated with CAG repeat number in the HTT gene. Greater than 26 repeats is not considered completely normal, with risk of passing on expansion to the next generation. The genetic test allows the identification of a fully penetrant mutation carrier during the preclinical stage, and the clinical diagnosis is made when unequivocal motor symptoms are present, but subtle motor signs, psychiatric symptoms, and cognitive changes may be present years before. Disease duration from first symptoms to complete care dependency and death is 15-20 years. Current therapeutic approaches are symptom driven, but investigational therapies that may slow or reverse disease progression are being studied. Early diagnosis remains important to provide genetic counseling and prompt access to symptom-relieving treatments, supportive care, and patient/family education.




















 English (US)
English (US)